Renal Ultrasound and Imaging: How to Evaluate Kidney Obstruction and Size
When your kidneys aren’t draining properly, time matters. Whether it’s a kidney stone blocking the ureter or a narrowing at the junction where the kidney meets the ureter, the first test your doctor will reach for isn’t a CT scan or an MRI-it’s a renal ultrasound. It’s quick, safe, and doesn’t use radiation. For patients with sudden flank pain, swelling, or a history of kidney issues, this simple scan can tell you if there’s a blockage, how bad it is, and whether your kidney is still working. Renal ultrasound works by sending high-frequency sound waves into your body. These waves bounce off your kidneys and bladder, creating real-time images on a screen. No needles, no contrast dye, no radiation. That’s why it’s the go-to test for pregnant women, kids, and anyone who needs repeat checks over time. But it’s not just about seeing the shape of your kidney. The real power lies in measuring its size, checking for swelling, and using Doppler to see how blood flows through it. Kidney size is one of the first things a sonographer looks at. In adults, a normal kidney is about 9 to 13 centimeters long. If one kidney is significantly smaller-say, under 8 cm-it could mean chronic damage from high blood pressure, diabetes, or long-term obstruction. A kidney that’s enlarged? That’s often a sign of something backing up, like urine trapped inside. The cortex, the outer layer of the kidney, should be at least 1 centimeter thick. If it’s thinner than that, your kidney’s filtering units may be scarred or shrinking. Then there’s the renal pelvis, the funnel-shaped area where urine collects before it flows down the ureter. A normal pelvis measures less than 7 millimeters across. If it’s wider, you’ve got hydronephrosis. This isn’t a diagnosis itself-it’s a sign. Hydronephrosis means urine isn’t draining well. The degree matters: mild, moderate, or severe. The Society for Fetal Urology system grades it from 0 to 4, and this helps doctors decide if surgery is needed or if it’s safe to wait. The real game-changer in renal ultrasound is the resistive index (RI). This isn’t just a number-it’s a clue to how hard your kidney is working against pressure. The RI is calculated from blood flow patterns in the arteries inside the kidney. You take the peak speed of blood flow during heart contraction, subtract the lowest speed during relaxation, then divide by the peak speed. Normal RI is below 0.70. If it’s 0.70 or higher, there’s a strong chance of obstruction. A 2015 study in the Nigerian Journal of Clinical Practice found that an RI of 0.70 or more was 86.7% accurate at spotting obstruction and 90% accurate at ruling it out. That’s better than many blood tests. But here’s the catch: RI can be misleading if you don’t know the context. A high RI can also happen in kidney infections, scarring, or even severe dehydration. That’s why you can’t look at the number alone. You have to look at the whole picture: the size of the kidney, the degree of hydronephrosis, whether both kidneys are affected, and how the patient feels. That’s why experience matters. A 2018 study found that novice sonographers could measure kidney length with up to 20% variation compared to experts. Training isn’t optional-you need at least 40 supervised exams to be reliable, according to the American Institute of Ultrasound in Medicine. Doppler ultrasound isn’t just for measuring resistance. It can also spot things you can’t see with the naked eye. For example, in ureteropelvic junction (UPJ) obstruction, a blood vessel might be crossing over and squeezing the ureter. Doppler helps find that. In kids, where UPJ obstruction is a common cause of hydronephrosis, Doppler is critical for deciding whether to monitor or operate. One urologist I spoke with said he tracks hydronephrosis weekly in post-op UPJ patients using bedside ultrasound instead of repeating CT scans. “No radiation, no cost, no wait,” he told me. “It’s the only way to manage this long-term.” Now, let’s talk about what ultrasound can’t do. It’s not great at spotting small kidney stones. If a stone is smaller than 3 millimeters, ultrasound might miss it. CT scans catch those every time. But CT exposes you to radiation-about 10 millisieverts per scan. That’s like 3 years of natural background radiation. For someone with recurrent stones, that adds up fast. That’s why guidelines from the American College of Radiology say ultrasound should come first. If ultrasound is negative but symptoms persist, then you go to CT. Magnetic resonance urography (MRU) gives you detailed pictures of the urinary tract and can show how urine flows, but it costs 3 to 5 times more than ultrasound. It’s also slower, noisier, and not always available. Nuclear scans can measure kidney function, but they use radioactive tracers. Again, radiation. So for most cases-especially initial evaluation-ultrasound wins. The biggest limitation? Obesity. If a patient has a BMI over 35, the sound waves can’t penetrate deeply enough. The image gets blurry, and measurements become unreliable. In those cases, you’re forced to use CT or MRU, even though they’re less ideal. A Mayo Clinic nephrologist told me in a 2021 survey that this is one of their biggest frustrations. “We’ll do the ultrasound, get a poor image, and have to schedule a CT. The patient’s upset. We’re upset. But we have no choice.” New tech is changing the game. Shear-wave elastography is now being used to measure how stiff the kidney tissue is. When urine backs up, pressure builds, and the tissue gets harder. Studies show stiffness increases linearly with obstruction. This could one day give us a number that tells us exactly how much pressure is building up inside the kidney-something we’ve never been able to measure non-invasively before. Another exciting development? Super-resolution ultrasound and ultrasound localization microscopy. These techniques can now visualize tiny blood vessels inside the kidney that were previously invisible. Researchers believe this could detect early signs of kidney damage from obstruction before any function is lost. It’s still experimental, but in the next 5 to 10 years, this could become standard. Artificial intelligence is also stepping in. At Mayo Clinic, they’re training AI to automatically grade hydronephrosis from ultrasound images. Right now, different radiologists can interpret the same image differently. AI could standardize that. One trial showed AI matched expert readings in 92% of cases. That’s huge for busy emergency departments where time is tight. In the U.S., about 12 million renal ultrasounds are done every year. Nearly every hospital has one. Emergency departments use point-of-care ultrasound to cut diagnosis time for kidney stones by 45 minutes. That’s 45 minutes less pain, less anxiety, and faster treatment. But it’s not magic. It’s a tool. And like any tool, it’s only as good as the person using it. If you’re being evaluated for kidney obstruction, here’s what to expect: No fasting. No prep. Just drink water normally. The scan takes 15 to 30 minutes. You’ll lie on your back or side while the tech moves a small probe over your flank and abdomen. They’ll take pictures, measure your kidneys, check for swelling, and run Doppler on the blood vessels. You’ll hear a whooshing sound-that’s the blood flow. You won’t feel anything. Afterward, your doctor will get a report with your kidney length, cortical thickness, pelvis width, hydronephrosis grade, and resistive index. If all numbers are normal, you probably don’t have a blockage. If the RI is high and the pelvis is dilated, you likely do. The next step? Maybe a CT scan to find the stone, or a referral to a urologist if it’s a structural issue like UPJ obstruction. The bottom line? Renal ultrasound isn’t perfect. But it’s the smartest first step. It’s safe, fast, and gives you more information than you think. It doesn’t just show you if there’s a blockage-it tells you how serious it is, how long it’s been there, and whether your kidney is still healthy enough to recover. For millions of people every year, it’s the difference between unnecessary radiation and a clear path forward. As technology keeps improving-with AI, elastography, and super-resolution imaging-ultrasound will only get better. But for now, its greatest strength remains simple: it lets you see inside the kidney without hurting it.
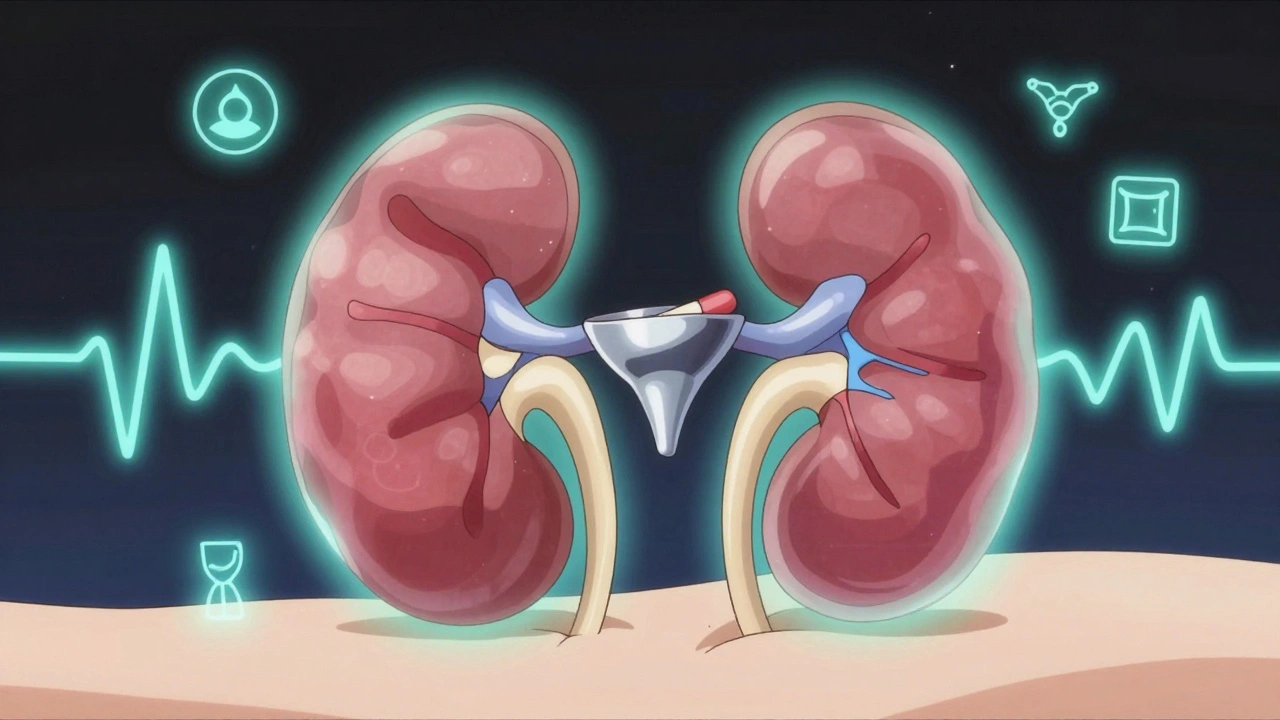
What does a normal renal ultrasound look like?
A normal renal ultrasound shows two kidneys that are symmetrical in size and shape. Each kidney measures between 9 and 13 cm in length. The cortex, the outer layer, is at least 1 cm thick and appears uniform in texture. The renal pelvis is narrow, less than 7 mm wide. No fluid collections or stones are visible. Doppler shows blood flow with a resistive index below 0.70, indicating no resistance to urine flow. The bladder is appropriately filled and emptying normally.
How accurate is ultrasound for detecting kidney stones?
Ultrasound detects about 80% of kidney stones larger than 3 mm. It’s less reliable for stones smaller than 2 mm, which are often missed. CT scans are more sensitive and can find stones as small as 1 mm. But because ultrasound doesn’t use radiation, it’s still the preferred first test, especially for young patients, pregnant women, and those with recurrent stones who need repeated imaging.
Can renal ultrasound show kidney function?
Standard ultrasound shows anatomy, not direct function. But when combined with Doppler, it can assess hemodynamic changes caused by obstruction. The resistive index (RI) reflects how much resistance blood flow faces inside the kidney. A high RI (≥0.70) suggests reduced blood flow due to pressure buildup from obstruction. While it doesn’t measure glomerular filtration rate (GFR) like a nuclear scan, it’s a strong indirect indicator of functional compromise.
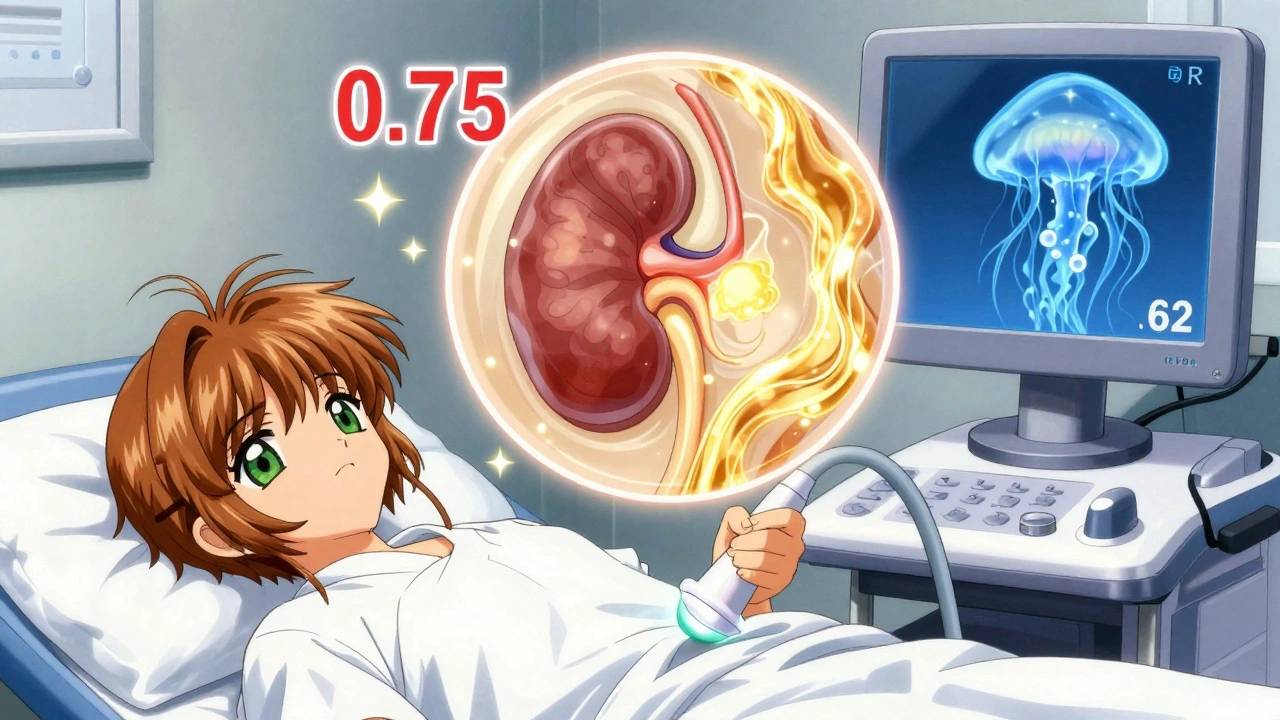
Why is the resistive index important in renal ultrasound?
The resistive index (RI) measures how easily blood flows through the kidney’s arteries. In obstruction, pressure builds up, compressing blood vessels and increasing resistance. An RI of 0.70 or higher is strongly associated with urinary obstruction. Studies show it has 86.7% sensitivity and 90% specificity for detecting obstruction. It’s not perfect-other conditions like infection or scarring can raise RI-but when combined with hydronephrosis and kidney size, it becomes a powerful diagnostic tool.
Can obesity affect the results of a renal ultrasound?
Yes. In patients with a BMI over 35, sound waves struggle to penetrate deep enough to get clear images of the kidneys. This can lead to inaccurate measurements of kidney size, cortical thickness, and hydronephrosis. In these cases, ultrasound may be unreliable, and doctors often have to switch to CT or MRI, despite their higher radiation or cost. This is one of the most common limitations cited by radiologists and nephrologists.
How often should someone get a renal ultrasound if they have hydronephrosis?
There’s no fixed schedule. For mild, stable hydronephrosis, monitoring every 6 to 12 months may be enough. For moderate to severe cases, especially after surgery or in children, weekly or biweekly scans may be needed to track changes. The goal is to see if the swelling is improving, staying the same, or getting worse. Ultrasound is ideal for this because it’s safe for repeated use. Many urologists rely on it to avoid repeated CT scans in patients with chronic obstruction.
James Kerr
Just had my first renal ultrasound last week for a weird flank pain-turns out it was just a tiny stone. No radiation, no needles, just a cold gel and some weird whooshing sounds. Felt like a sci-fi movie but way less scary. 😅
Albert Essel
The article accurately captures the clinical utility of renal ultrasound as a first-line modality. The resistive index, while not diagnostic in isolation, provides valuable hemodynamic insight when correlated with anatomical findings such as hydronephrosis and cortical thickness. Its specificity for obstruction is clinically significant, particularly in resource-limited or radiation-sensitive populations.
Charles Moore
Really appreciate how this breaks down a complex topic without dumbing it down. I'm a med student in Dublin and we’re just starting ultrasound rotations-this is gold. The part about Doppler spotting vascular compression in UPJ obstruction? That’s the kind of detail that makes you go ‘whoa.’
Gavin Boyne
So let me get this straight-we have AI that can read kidney ultrasounds better than some radiologists, yet we still make patients wait 3 weeks for an appointment because ‘we need to schedule it properly.’ Classic American healthcare: cutting-edge tech, middle ages logistics. 🤡
Rashi Taliyan
My cousin got diagnosed with hydronephrosis after her third pregnancy-she was terrified, but the ultrasound saved her. No radiation, no scary needles, just a gentle tech who explained everything. Now she checks in every 4 months with a quick scan. It’s not perfect, but it’s gentle. And that matters so much.
Kara Bysterbusch
What strikes me most is not merely the technological sophistication of Doppler resistive index measurement, but the profound philosophical implication: we are now able to quantify the silent pressure within the human body-not through invasive catheters or radioactive tracers, but through the elegant physics of sound waves. This is medicine evolving toward non-invasive empathy.
Rashmin Patel
OMG I can’t believe people still think CT is the go-to for kidney stones?? 😱 I had a 4mm stone last year and did 3 ultrasounds over 6 weeks-no radiation, no cost, no drama. My urologist even showed me the video of the stone moving! Super-resolution ultrasound? AI grading? YES PLEASE. We need this everywhere, especially in India where CT scans are expensive and radiation exposure is a real concern for families. Why are we still clinging to outdated tech? 🙏
sagar bhute
This article is a textbook example of medical propaganda. Ultrasound misses stones. It’s unreliable in obese patients. It’s operator-dependent. And now you’re telling me AI will fix it? Please. The real problem is that hospitals are underfunded and radiologists are overworked. No amount of fancy Doppler or elastography will fix that. Stop pretending tech is the solution when the system is broken.
Cindy Lopez
Wow. 12 million renal ultrasounds a year. And not one of them was done by someone who actually knew what they were looking at.